

There was a debate between PZ Myers, David Brin, Eliezer Yudkowski and Eneasz Brodski about immortality. Eliezer brought up the point about different levels of immortality and had 10,000 years as a lower bound of immortality. Many of the complaints from PZ Myer and David Brin were concerns about societal effects that might accompany the change to people living a lot longer.
I would point out that any radical life extension that extended healthy living to about 250 or 300 years of age would have the same societal effect for the next 100-120 years as any life extension beyond that level. The reason being is that the oldest people are now 115 years of age. If the extension or rejuvenation procedures are successful and people are enabled to live significantly longer, the people will still be adding years of life one year at a time. There would not be people living to an aged end of life for say the first 80% of the extended life or perhaps all but the last 20 years.
This also means that extending lives to about 160 to 180 years with a moderate amount of rejuvenation would have the same societal effect for the next 40 years.
The exact effect on individuals would vary depending upon how lives were extended. However, societally it would look the same as for a number of years and decades all of the people who received treatments.
Vaccination and clean water extend lives
The method of life extension will determine costs and the rate deployment and adoption. How quickly the method can be adopted by the most people will determine the level of societal impact.
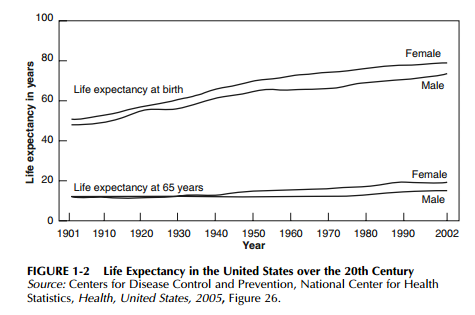
Current best public health (universal vaccination, clean water, adequate food, clean sanitation, prenatal/natal and basic care of children up to the age of 5) if universally adopted would enable everyone to have a life expectancy over 70 years of age.
Global coverage with three doses of the diphtheria-tetanus-pertussis vaccine by 12 months of age (DTP3) rise from 5% in 1974 to 85% in 2010. However, sub-Saharan Africa reached only 77% DTP3 coverage in 2010
Vaccines can increase life expectancy by protecting against diseases against which one would not expect benefit. Elderly individuals given influenza vaccine in the USA had approximately 20% less chance of suffering cardiovascular and cerebrovascular disease and 50% lower risk of mortality from all causes compared to their unvaccinated counterparts.
In Sweden, administration of polysaccharide pneumococcal vaccine and inactivated influenza vaccine significantly reduced the risk of in-hospital mortality for pneumonia and cardiac failure among elderly persons, with an additive effect when both vaccines had been administered.
By reducing the need for antibiotics, vaccines may reduce the prevalence and hinder the development of resistant strains. Introduction of a conjugate pneumococcal vaccine for infants in the USA in 2000 saw a 57% decline in invasive disease caused by penicillin-resistant strains and a 59% decline in strains resistant to multiple antibiotics by 2004 across a broad age spectrum: 81% among children under 2 years of age and 49% among persons aged 65 years and older.
25 years of life extension in the UK from 1979 to 2003
Brock (2006) reports on mortality developments in different age groups in the UK for the period from 1979 to 2003:
* Infant mortality rates fell by nearly 60% (cause of death not available due to a change in registration
certificate).
* Ages 1 to 14: mortality fell by 57% for boys and 50% for girls, with injury and poisoning rates (the highest cause in 1979) almost halved.
* Ages 15 to 44: for young men, injury and poisoning (by far the highest cause of death) fell only gradually, whereas for young women cancer (the biggest killer) fell by 45%.
* Ages 45-64: circulatory disease was by far the biggest killer of men at the beginning of the period, and the death rate fell by two-thirds, leaving cancer as the biggest killer, despite the death rate for cancer falling by 34%. For women cancer accounted for almost half of all deaths, and circulatory diseases for almost a third. Both causes declined over the period: cancer by 29% and circulatory diseases by 65%.
* Ages 65-84: age-standardised death rates fell by around 40% for men and a third for women. The predominant cause of death for both men and women was circulatory diseases, and the death rate for both sexes fell by 55% over the period. Cancer (but of different types) was the second biggest killer for both sexes, with death rates declining for men but not noticeably for women.
* Ages 85 and over: circulatory diseases and respiratory diseases were the biggest killers, and both declined substantially over the period.
World life expectancy increased by about 5 years from 1990 to today and increased by 7 years in the 1960s

Preventing or curing cardiovascular disease, cancer and Alzheimers and other general life improvements should get life expectancy up to about 90-100 years
Effect early detection of cancer would enable far more effective treatments against the earliest stages of cancer.
If we are able to transfer the genetic immunity that some people have to diseases could enable the major diseases to be neglible for world public health.
Only medical treatments with the cost profiles of clean water and vaccination will become truly universal before at least 2035
It is taking until about 2025 to make vaccination truly universal. So any new medical or public health treatment would need to not be more costly or difficult to deploy until at least 2035.
Significant life extension possibilities
SENS repair of aging damage. The estimates are that it would add 30 years to maximum lifespan. It would be quite expensive initially and then could be adopted into the developed world’s national health systems over perhaps 10-20 years. Any SENS procedure costs would be displacing and delaying the need for the expensive medical procedures associated with end of life diseases. SENS is going to 4 million per year of funding and in 5 years could be at the $10-25 million per year funding level. Human SENS treatments could arrive in the 15-35 year timeframe.
Telomere extension (immortalized cells), stem cells and tissue engineering. There is the possibility significant progress and efforts towards life extension with stem cells and tissue engineering. I think significant treatments could arise in this area in the 5-25 year timeframe. These procedures look like they would remain relatively costly. However, a global middle class where everyone has over PPP $30,000 per person could be achievable for 75% of the world population by about 2035 and 90% of the world population by about 2045.
An intensive surgery procedure that could be combined with stem cell and synthetic biology neuron rejuvenation is full body transplantation. This would likely remain very expensive even with massive adoption of more advanced and affordable robotic surgery. How much would people complain about massively costly and invasive treatments for life extension of the elite ? An example is Dick Cheney received a heart pump in 2010 and has had more than one bypass operation since 1988 and had an implantation of an implantable cardioverter-defibrillator in June, 2001. Cheney also had a heart transplant in 2012. Only a very wealthy person could have undergone this level of treatment to add 25 years and counting. It appears that Cheney could last another ten years for a total of 35 years as the result of privileged medical treatment levels.
George Church is working on synthetic biology approaches to achieving indefinite lifespans. George’s idea is to bring in sections of DNA from exotic organisms or genes that are rare for humans to enable all people to have desired genetic capabilities. He describes capabilities such as immunity to all viruses and cellular immunity to radiation and creating immunity to diseases. They are working to sequence and determine the genetic basis for long lived animals and humans and determine how to engineer longer lived people. They are working on approaches to rejuvenate different kinds of cells including the neurons of the brain.
Synthetic biology costs are rapidly falling, so success in this area could rapidly become affordable after the initial development.
George has had a number of commercial successes using synthetic biology to develop biofuels and industrial products. The costs and precision of gene synthesis and gene therapy are rapidly falling (falling faster than Moore’s law lowering the cost of electronics). I think significant treatments could arise from the synthetic biology area in the 7 to 30 year timeframe.
Molecular nanotechnology has the potential to enable radically improved nanomedicine. Molecular nanotechnology could be used to make any SENS therapies more effective and could enhance the effectiveness and affordability of synthetic biology. There are significant capabilities now with DNA nanotechnology. I believe that full blown molecular nanotechnology will be developed in 10-40 years.
Countries now with life expectancy at about 80 or higher
Note that there is also nearly a 100% gap between the longest lived people and the shortest. The shortest have life expectancy in the 40s while many people have life expectancy in the 80s and even 90s (some sub-populations). Medical treatment and wealth enables wealthier people to live 6 years longer within the same country and 30 years longer between countries. There has not been global or national unrest related to that particular topic. There have been demonstrations like the occupy movement and economic injustice but not specifically focused on life extending medicine. There are some demonstrations and political movements for access to medical care but those are a fraction of the amount for jobs or to protect jobs or against high food prices.

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.