

Fightaging summarizes the lengthy Chronopause article.
[For example], mature, clinically available, and FDA-approved therapies to slow or halt brain cell loss are a decade, and likely closer to two decades, away. And when clinical application does come, it will likely be only for the most serious disease states, such as [Alzheimer’s disease], Huntington’s Disease (HD), and Amyotrophic Lateral Sclerosis (ALS). Even in these conditions, access to treatment may be limited by many factors, including high cost and government regulation. Thus, for many of us, even another decade of waiting will be too long. … One of the hardest things for people to understand is that it is possible to do good, without doing good enough; and nowhere is this more the case than in medical research
COURAGE and the ability to understand that human experimentation, preferably by those with the most to lose and the most to gain, is the only path to the development of fast and effective therapies. Animals are not people, just as certainly as people are not animals: and while animal research can provide useful leads, and help to explicate the mechanics of both disease processes and therapies, it is no substitute for human experimentation. The increasing absence of the latter has arguably become one of the most critical elements in slowing medical progress today.
Twenty years ago, gay men dying in droves from a bizarre and unprecedented illness made the decision that AIDS research was too important to be left to the mainstream government and big Pharma scientists. Instead, they took personal responsibility for their plight, organized, mobilized, agitated, and struck out on their own in search not just of a cure, but for any treatment that offered the real prospect of longer life, or a reduced disease burden. They achieved amazing things, because they knew they were dying NOW, and because they also well understood that the society they were embedded in fundamentally didn’t give a damn about them – or their priorities. Cryonicists and those who support extreme longevity are in exactly the same position today.
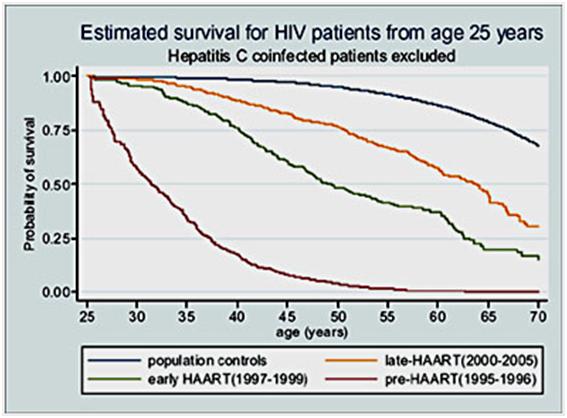
However, the analogy with AIDS cannot be completely sustained, because the median survival rate after diagnosis of AIDS before the advent of HAART typically only ~ 6 months to 2 years. Something which added a sense of urgency most likely not shared by those effected by brain aging, including cryonicists. I suspect that the personal and cultural traits of the male gay community culture are more conducive to pursuing such an aggressive and effective course of action than are the traits of the typical cryonicist, but serious call to arms might still be successful.
Certainly it is disheartening to see projects like this one, Research Project 2010b – Microglia Stem Cells: http://www.imminst.org/Research2010B, being funded by the Immortality Institute. This study is described as aiming to “to replace non-functional microglia with new and young microglia cells derived from adult stem cells. We will inject these young microglia cells into ‘Alzheimer mice’- a model for Alzheimer’s disease. After giving the cells some time to work, we will sacrifice the mice and measure microglia activity, neurogenesis, proliferation of neuroprogenitors and plaque density in the brain. A reduction in plaque density of Alzheimer mice would be a first proof that the transplanted microglia are performing their expected function.” It is disheartening not because this isn’t important and worthwhile work, but rather because it is scientific research of the kind that is being well funded by large, well established governmental and NGO research entities, with disease-specific agendas. A quick perusal of Pubmed shows these studies (very similar in design, therapeutic mechanism, and objectives) to have been already undertaken and completed. These are the very entities who have been trying (unsuccessfully) to cure cancer heart disease, muscular dystrophy and multiple sclerosis, for decades having expended billions of dollars in taxpayers’ and charitable givers’ money with little to show in the way of progress.
If “Research Project 2010b” were completed successfully in 5 years or even in 3 years, it would still produce no results that will do anything to stop the 1 per second, 85,000 per day, or ~31 million per year brain cells you and I are losing right now – not to mention the concurrent staggering loss in neuronal and glial cell mass and function. What’s more, treatments such as these are invasive, require extraordinarily skilled practitioners to deliver the therapeutic cells to the targeted areas of the brain, carry the risk of serious (surgical) adverse events, and will cost a fortune. They also will require FDA approval and the approval of the medical infrastructure for their application – an infrastructure that does not even recognize aging as a disease and is not going to do so anytime soon. This is wonderful research, but it is research of the kind that was not undertaken by AIDS activists, and that typifies why AIDS was made a controlled and highly manageable condition whilst other, far less complex and equally devastating diseases, remain untreatable. Project 2010b is Big Medicine, disease-specific research that, at least in my opinion, is one of the last places cryonicists, and others who are trying to stay alive and cognitively healthy now, should put their time, their effort, or their money into.
Rather, we should look to the paradigm that brought HIV/AIDS, a fundamentally new and extraordinarily complex disease, to its knees in a scant 14 years. That paradigm focuses on identifying, funding and executing projects which offer the prospect of immediate intervention that can make material differences in the clinical condition of patients (us!) in the shortest possible time. With the advent of sophisticated brain imaging technology, and indeed even using far simpler, standard clinical MRI, as well as sophisticated psychological neurocognitive testing, such as has been developed by Salthouse and his colleagues,176 it is possible, right now, to begin evaluating the large and rapidly growing pool of molecules, both singly and in combination, that have been demonstrated to slow, and in some cases reverse, both the structural and functional neurocognitive decline associated with so-called ‘healthy aging.’
Instead of the alarmingly reckless, arbitrary, and feedback-free self experimentation that is seen with great frequency on the Immortality Institute Forums, and other life extension-related list-serves, there should be a well designed and well coordinated program of both animal and human experimentation to identify pharmacological interventions that are actually proven to slow, halt, or reverse neurocognitive decline. The imaging technology and the neurocognitive testing (much of which can be administered at a distance using a PC and the Internet) that are now both available and affordable, should be immediately pressed into service to validate the efficacy, or lack thereof, of these potentially powerful therapeutic molecules. If we had nothing more sophisticated or promising than that old standby for the treatment of bipolar disorder, lithium carbonate, such research would be more than justified. But there are many promising and (so far) largely adverse effect free molecules, that cry out for further animal evaluation, followed by rapid application to those of us humans willing to take the risks – risks that I believe are wholly acceptable within the context of a well designed program of self-experimentation (with careful monitoring for both efficacy, and for the emergence of adverse effects).
If you liked this article, please give it a quick review on ycombinator or StumbleUpon. Thanks

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.