

World Health Organization – Global Health Risks report from 2009 (70 pages)
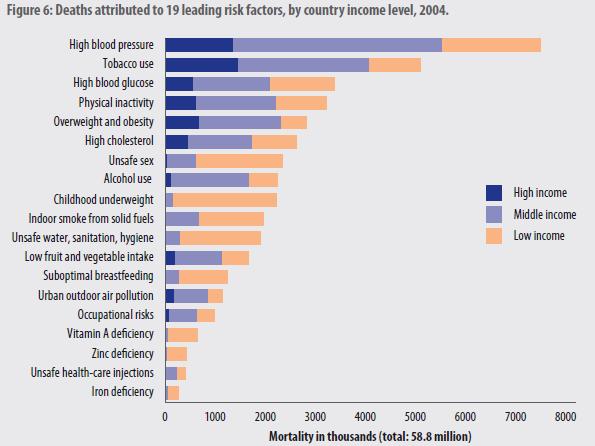
The leading global risks for mortality in the world are high blood pressure (responsible for 13% of deaths globally), tobacco use (9%), high blood glucose (6%), physical inactivity (6%), and overweight and obesity (5%). These risks are responsible for raising the risk of chronic diseases such as heart disease, diabetes and cancers. They affect countries across all income groups: high, middle and low. The leading global risks for burden of disease as measured in disability-adjusted life years (DALYs) are underweight (6% of global DALYs) and unsafe sex (5%), followed by alcohol use (5%) and unsafe water, sanitation and hygiene (4%).
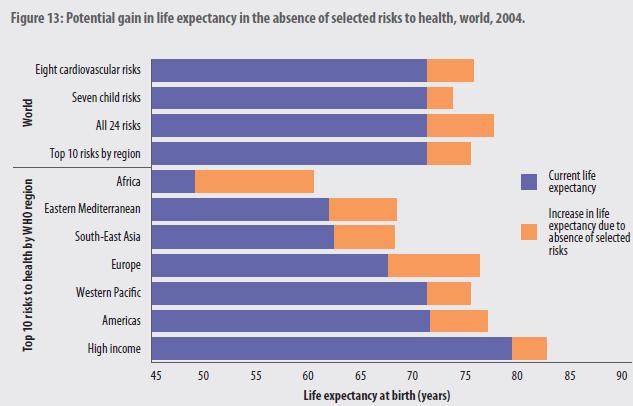
World life expectancy would go up by about seven to ten years if all of the primary global health risks were eliminated. Life expectancy in high income countries would go up by about 2 to 3 years.
Air Pollution – Particulates are the easiest to quantify and have the best evidence
Correcting a previous article: For the amount of lives that could be saved from air pollution to equal the world war 2 combat deaths would require fixing indoor air pollution and particulates for outdoor air pollution. Although air pollution deaths are likely underestimated because there are effects from other pollutants but the evidence and causal relationships have not been conclusively defined.

From 2002 (link to spreadsheet by country), figures were 2.4 million deaths total from air pollution (although this figure does not include new associations with peristent free radicals). From 2002, 865,000 deaths from outdoor PM10 air pollution. So indoor and outdoor did not add to 4 million deaths.
An updated World Health Organization statement from 2010 on air pollution.
In the year 2004, indoor air pollution from solid fuel use was responsible for almost 2 million deaths (3% of all deaths) and 2.7% of the global burden of disease (expressed in disability-adjusted life years, or DALYs*). This risk factor is the second largest environmental contributor to ill-health, behind the combination of unsafe water with poor sanitation. In low- and middle-income countries, 3.9% of all deaths are due to indoor air pollution.Worldwide, indoor smoke from solid fuel combustion causes about 21% of deaths from lower respiratory infections, 35% of deaths from chronic obstructive pulmonary disease and about 3% of deaths from lung cancer.
In the year 2004, outdoor air pollution in urban areas was responsible for almost 1.2 million deaths (2% of all deaths) and 0.6% of the global burden of disease. Transportation-related air pollution, which is a significant contributor to total urban air pollution, increases the risks of cardiopulmonary-related deaths and non-allergic respiratory disease. Some evidence supports an association of transportation-related air pollution with increased risks of lung cancer, myocardial infarction, increased inflammatory response and adverse pregnancy outcomes (e.g. premature birth and low birth weight).
Exposure to particulate matter, including metals, has been linked to a range of adverse health outcomes, including modest transient changes in the respiratory tract and impaired pulmonary function, increased risk of symptoms requiring emergency room or hospital treatment, and increased risk of death from cardiovascular and respiratory diseases or lung cancer. Particulate matter is estimated to cause about 8% of deaths from lung cancer, 5% of deaths from cardiopulmonary disease and about 3% of deaths from respiratory infections.
Another air pollution disease burden study from 2005
The impact of outdoor air pollution on the burden of disease in the world’s cities is large, but an assessment of sources of uncertainty, including the fact that only mortality impacts of exposure to PM were estimated, suggests that the impact is actually underestimated.
As a consequence of the uncertainties in this global assessment, its quantitative
results cannot be confidently extrapolated to smaller geographic areas, such as specific countries or cities. The methods for estimation of exposure and extrapolation of concentration-response functions were developed specifically for estimating burdens for large geographic regions, often in the absence of essential data on exposure and response.
Outdoor PM air pollution is estimated to be responsible for about 3% of adult cardiopulmonary disease mortality; about 5% of trachea, bronchus, and lung cancer mortality; and about 1% of mortality in children from acute respiratory infection in urban areas worldwide. This amounts to about 0.80 million (1.2%) premature deaths and 6.4 million (0.5%) lost life years.
The burden of disease due to urban air pollution occurs predominantly in developing countries; developing Asia is estimated to contribute approximately two-thirds of the global burden. Moreover, the burden of air pollution from all sources considered in the CRA (indoor, outdoor, occupational, and lead) accounts for about 1.9 million premature deaths annually, about 5.4% of the total disease burden in the 3 regions in terms of DALYs (Health Effects Institute [HEI], 2004). This burden is quite noteworthy: it is, for example, half again as much as that of tobacco and twice that of unsafe sex (due to acquired immunodeficiency syndrome and other risks) (WHO, 2002).
NASA had some recent work on PM2.5 health risks and where the pollution in globally and in the United States. The 2002 data from the World Health Organization is for 10 micron particulate matter, and does not include the newer work on 2.5 micron particulate matter.
The American Heart Association estimates that in the United States alone, PM2.5 air pollution spark some 60,000 deaths a year. Though PM2.5 as a class of particle clearly poses health problems, researchers have had less success assigning blame to specific types of particles. “There are still big debates about which type of particle is the most toxic,” said Pope. “We’re not sure whether it’s the sulfates, or the nitrates, or even fine dust that’s the most problematic.”
One of the big sticking points: PM2.5 particles frequently mix and create hybrid particles, making it difficult for both satellite and ground-based instruments to parse out the individual effects of the particles
Particulate Matter Air Pollution and Cardiovascular Disease (2010)
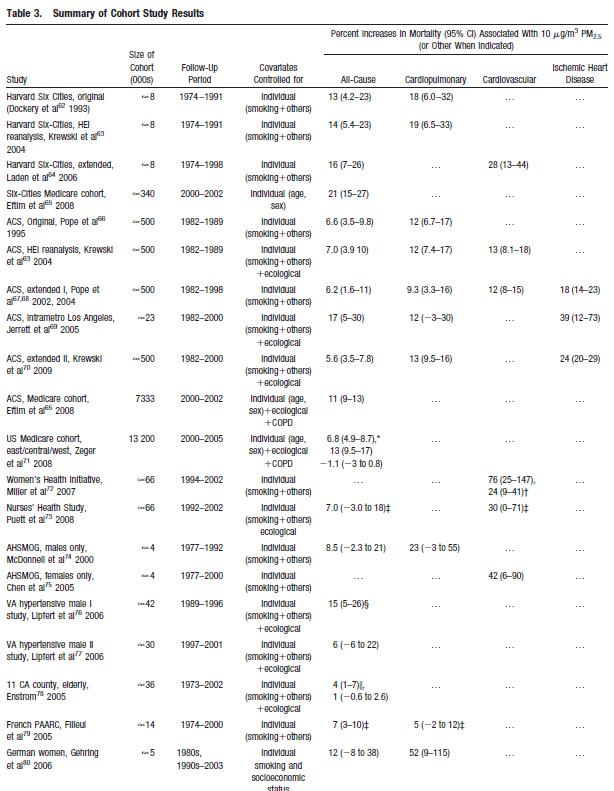
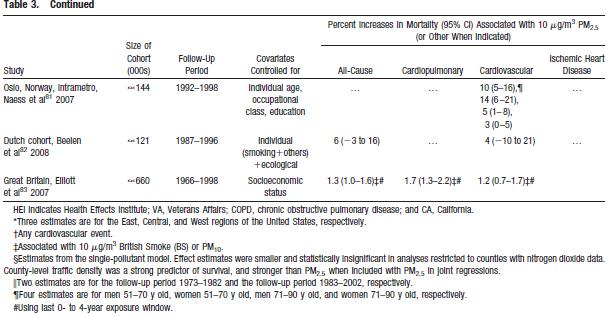
Click for a larger view of this table summarizing the air pollution studies on health impacts

The overall evidence from the cohort studies demonstrates on average an approximate 10% increase in all-cause mortality per 10-micrograms/m3 elevation in long-term average PM2.5 exposure.
Excess cardiovascular mortality and increased rates of hospitalizations are similarly associated with day-to-day changes in PM air pollution. However, significant differences between geographic regions in the risk relationships have been observed, and more investigation is required to explain this heterogeneity.
Global Health Risks


If you liked this article, please give it a quick review on ycombinator or StumbleUpon. Thanks

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.